
Flueck Joëlle Leonie
Swiss Sports Nutrition Society, Affoltern am Albis, Switzerland
Abstract
The relative energy deficiency in sport (REDs) is a complex state of low energy availability in the athletes’ body. Signs and symptoms comprise not only a low bone mineral density and a menstrual dysfunction as initially thought but also a metabolic and hormonal imbalance together with cardiovascular and mental issues. This leads to an increased risk for injury and illness and decreases performance over a longterm. In this review the complexity of the issue together with some suggestions for underlying causes are summarized. Furthermore, some aspects on nutritional interventions in the case of low energy availability are suggested. Some proposition how to work in an interdisciplinary team together with the athlete and the social environment were pointed out. In the future, distinct protocols are needed for the correct diagnosis of this health-issue. Furthermore, prevention strategies are desperately required to prevent as many athletes as possible from low energy availability.
Zusammenfassung
Das relative Energiedefizit im Sport (REDs) ist ein komplexer Zustand geringer Energieverfügbarkeit im Körper der Athlet*innen. Zu den Anzeichen und Symptomen gehören nicht nur eine niedrige Knochendichte und eine Zyklusstörung, wie ursprünglich angenommen, sondern auch ein metabolisches und hormonelles Ungleichgewicht sowie kardiovaskuläre und psychische Probleme. Dies führt zu einem erhöhten Verletzungs- und Infektionsrisiko und vermindert langfristig die Leistungsfähigkeit. In dieser Übersicht werden die Komplexität des Themas und einige Vorschläge für die zugrundeliegenden Ursachen zusammengefasst. Darüber hinaus werden einige Aspekte zu Ernährungsinterventionen bei geringer Energieverfügbarkeit zusammengefasst. Auch die interdisziplinäre Zusammenarbeit zusammen mit den Athlet*innen und deren sozialem Umfeld ist von hoher Wichtigkeit. Für die Zukunft werden eindeutige Protokolle für die korrekte Diagnose dieses Gesundheitsproblems benötigt. Darüber hinaus sind Präventionsstrategien dringend erforderlich, um möglichst viele Athlet*innen vor einer geringen Energieverfügbarkeit zu bewahren.
Schlüsselwörter: Sporternährung, Energieverfügbarkeit, Leistung
Introduction
Protecting the health of athletes must be one of the primary goals of the International Olympic Committee (IOC) but of course also of all the practitioners whether from sports medicine, psychology, physiotherapy or nutrition. In the 2005 IOC Consensus Statement, “The Female Athlete Triad” was described as a combination of an eating disorder or disordered eating pattern and irregular menstruation that could lead to adverse health effects on various body functions [1]. It was explained that endogenous oestrogen levels and other hormones could be disturbed, as well as a reduction in bone mineral density would occur [2]. Over time, scientific evidence has shown that other health issues are closely linked to low energy availability [3]. If an athlete expands a high amount of energy through training volume or intensity and does not fuel sufficiently, a low energy availability will result. But also athletes with a lower training volume but a very low energy intake might be affected. Not only hormonal imbalance and low bone mineral density are resulting from this situation, but also other important functions such as immune function, muscle protein synthesis, cardiovascular and mental health are impaired [3,4]. Furthermore, low energy availability does not solely occur in female athletes, it includes male athletes as well. Therefore, in 2014, the wide range of symptoms around low energy availability were renamed from “Female Athlete Triad” to relative energy deficiency in sport (REDs). Figure 1 shows the various different effects of low energy availability on physiological functioning of the body which can lead to massive health problems and a decrease in performance.

Incidence of low energy availability
Not every case of low energy availabilty has an underlying eating disorder or a disordered eating pattern. This has been nicely summarized by Wells et al. 2020 [5]. Some of the athletes are also just unprepared regarding food provision during a busy training or school day or exercise to a very high extent, that caloric requirements can’t be matched. Nevertheless, eating disorders are very common in elite sports. Between 13 and 20% of women and 3 to 8% of men are affected [4]. Furthermore, athletes are also at risk for exercise addiction [6]. How high the incidence in the various sports is depends on the sport itself. Aesthetic sports such as rhythmic gymnastics, ballet dancing or figure skating as well as endurance sports such as long-distance running, cross-country skiing, triathlon and road cycling are the sports with a frequent occurrence of low energy availability and/or eating disorders in men and women. But also sports climbing, ski jumping or ski mountaineering are sports with a very high risk.
Definition of low energy availability
The term energy availability describes the available energy when substracting the energy expenditure through training from the daily energy intake in relation to the fat-free mass. It is known, that some minimal energy requirements are needed to keep all the physiological functions of the body working optimally. If the energy level is too low, than our body will be required to spare some energy somewhere. Mostly, this will be done by shuttin down some body functions for example reproductive function, which is not “essential” in this situation to survive. The following equation can be used to estimate energy availability:

It seems quite hard to accurately determine energy availability in “real life” [7]. Nevertheless, in practice, the estimation of energy availability might give some further information about the energy status of an athlete. To calculate energy availability, a precise food and training diary over 3 to 7 days has to be recorded. Based on it, the daily energy intake and exercise energy expenditure can be estimated together with some other performance-related data (e.g. heart rate, ergospirometric data). For the calculation of fat-free mass, a dual X-ray absorptiometry (DXA) measurement is usually used to determine body composition [8,9]. It should be noted, however, that the calculation of energy availability can be subject to error (over-/underestimation of energy intake and exercise energy expenditure) and should therefore, never be used as the sole diagnostic tool [7].
Together with some further medical examination and biomarkers such as hormonal and menstrual function and bone mineral density, it might be possible to diagnose an athlete with REDs. Studies have shown, that in female athletes, an energy availability below 30 kcal/kg fatfree mass/d led to serious health implications and was classified as a low energy availability. Whether this cut-off value applies for male athletes as well has to be determined in the future. Values around 40 to 45 kcal/kg FFM/d seem to be sufficient in terms of providing enough energy to keep essential body functions such as reproductive system or bone health in a good spot. On the other hand, it seems also obvious, that at certein time points during an athletic season, body composition might be optimized to achieve maximal performance. But even there, a severe low energy availability over a very short-term period of several days, might already affect some of the health-related parameters and also diminish performance [10].
Nutritional aspects leading to low energy availability
Eating habits, pressure to perform, high training volume and intensity, together with a thrive to optimize body composition are all factors that can cause an imbalance in energy balance and thus potentially lead to low energy availability. For example, eating disorders, a massive caloric restriction and a rapid weight loss are risk factors. However, an eating disorder or disturbed eating behaviour is not always the underlying cause. Ignorance, poor nutrition planning or a high fibre content in the diet can also be the reason for [5,11]. Other factors such as mental health, the influence from family, friends and peers or through social media, socio-economic and genetic factors also play a decisive role [12]. In addition, diets that are intended to increase performance, pressure to lose weight, overtraining or recurring injuries can affect eating behaviour and thus also energy availability [13]. Furthermore, a low energy availability can also occur unconsciously, as a result of training with very high volumes or at high intensity and not being able to supply sufficient energy through food intake. The effect of exercise on appetite regulation and the feeling of hunger must also be taken into account [14].
Signs and symptoms of relative energy deficiency in sport
The effects of low energy availability are very far-reaching and depend on how long one has been in this imbalance (Figure 1). For example, athletes who have been suffering from low energy availability for a long time often show micronutrient deficiencies such as iron deficiencies [15]. Even a high cholesterol seems to be related to it [16]. But as mentioned before, also a decreased bone health leading to osteopenia or even osteoporosis is often detected. Moreover, systemic inflammation seems to be increased and together with low energy intake and chronic fatigue this can lead to an increased risk for infections and injuries [1]. Stress fractures are often seen in high-impact sports such as running [15]. Therefore, the injury history of an individual is also very important to properly diagnose a REDs. Other physiological and medical complications affect the cardiovascular system, gastrointestinal discomfort, a reduced muscle protein synthesis [17,18], hormonal imbalance and a reduced reproductive function
[19, 20]. Even a causal relation between urinary incontinence and low energy availability has been shown more recently [21]. In addition, psychological stress can be a further reason for low energy availability, but also a health issue resulting from it.
Screening and diagnosis
The screening and diagnosis of a relative energy deficit is very complex and requires an interdisciplinary team around the athlete. Early detection of the problem in particular can help to avoid further health implications and stabilise performance in the long term. It might be important to monitor factors such as changes in eating behaviour, growth and maturation in younger athletes, menstrual function and cycle length, recurrent injuries and illnesses and mood swings. Furthermore, if a REDs is suspected, additional health parameters such as thyroid function (T3), heart function (ECG), cholesterol, leptin and testosterone levels in male athletes might give some further information [20,22]. Also, the assessment of bone mineral density is needed. The use of different questionnaires might help to detect signs of eating disorders or disturbed eating behaviour [23] toghether with information about mental health and exercise additction [6]. However, a proper diagnosis of an eating disorder can only be made by a specialist in psychology or psychiatry. Furthermore, the measurement of resting energy expenditure (in the morning, fasted) can be used complementary as a diagnostic and monitoring tool. In the case of a low energy availability, the metabolism is slowing down to spare energy [20,24]. It has been shown, that the ratio between measured and predicted resting energy expenditure was less than 0.90 in females with REDs [24-26]. However, factors including varying states for energy balance but also food intake and exercise may influence the assessment [26]. Therefore, a standardized and valid measurement is needed to include this parameter into diagnosis.
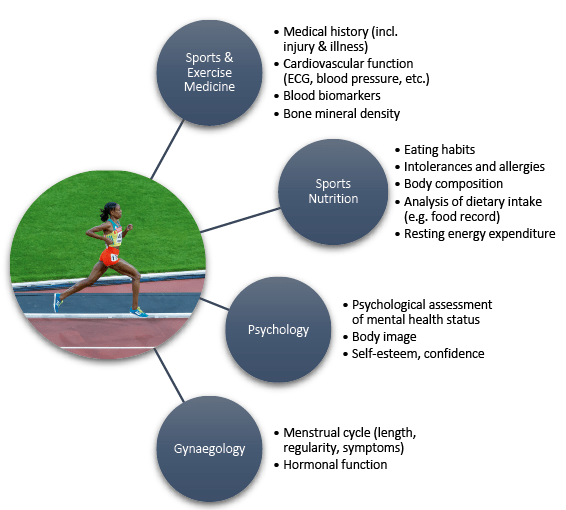
All these examinations, as well as the athlete’s complete medical and family history, can help to make a comprehensive and evidence-based decision about the underlying cause of the symptoms. Already in the screening phase, it is worthwhile to build an interdisciplinary team around the well-being of the athlete (Figure 2). This allows a specialist to screen the overall nutritional habits (specialist in sports nutrition), the menstrual cycle and hormonal fluctuations (specialist in gynaecology), medical and injury history, laboratory biomarkers, ECG, bone mineral density and health status (sports and exercise physician) as well as a differentiated psychological assessment of the overall situation (psychologist). This interdisciplinary approach allows for a broad perspective before formulating a diagnosis but also helps to conclude together with the athlete, his family and the coaching staff for the best and most effective treament strategy.
Treatment of low energy availability: the nutritional perspective
Treatment of low energy availability usually involves increasing energy intake, reducing stress and energy expenditure, or a combination of all three [4,11]. In the absence of menstruation, an increase in body mass seems to be a crucial factor in restoring normal function of the reproductive organs [25,27]. The extent of weight gain until the onset of regular menstrual function cannot be predicted. An individual therapy plan seems to be necessary. Again, an adequate daily intake of protein, fat and carbohydrates plays an important role [28,29]. Furthermore, timing of the nutritional intake seems to be another important factor as within-day low energy availability might occur [30]. Especially, ensuring an adequate energy intake around training sessions as well as consuming breakfast and dinner are significant. Moreover, incerasing carbohydrate intake can further help to restore body functions [11]. Additionally, it has been shown, that female athletes with oligomenorrhea had a higher dietary fiber intake compared to eumenorrheic athletes [31]. Thus, high amounts of fiber-containing foods might limit energy intake. Therefore, in some cases, low-fiber alternatives might be more appropriate to increase energy intake [11].
Various strategies can be used to improve bone health. First of all, an adequate energy intake is crucial. In addition, specific exercises which increase the mechanical load on the bones (e.g. jumps and exercises with higher impact) can help to increase bone mineral density [11]. A sufficient supply of vitamin D and calcium are necessary, especially if a low calcium intake and a vitamin D deficiency are present. It is recommended to check the vitamin D status and, if necessary, supplement [32]. Bone mineral density is equally important in male and female athletes. Especially in low-impact sports such as swimming or cycling, low bone mineral density is often found in male athletes as well.
Often, the athletes do not want to admit, that there is a problem with energy supply and body image issues which makes it hard for them to accept the reality. A resistant behaviour can be a sign for an eating disorder [33]. It is advisable to seek the cooperation with a specialist in the field of psychology. But first of all, the athlete has to agree with it. Often, time and building trust is needed before they accept. Furthermore, if the athletes gives the permission, it can also help to include close family members, friends or the coach into therapy. This might be beneficial for the long-term success of the intervention.

Conclusion
From the available literature, it seems obvious that a high a amount of athletes is affected by REDs. However, more studies are needed to improve diagnosis but also prevention. There is a huge potential to minimise REDs-related health issues if education and prevention on REDs get a higher importance in professional sports. Sports associations need to build a network of medical experts, not only in sports and exercise medicine or physiotherapy, but also in sports nutrition and psychology. The interdisciplinarity of such a medical team would be good step into the right direction. This team would be needed to raise the awareness of negative effects of low energy availability. But also an update of best-practice protocols and the elimination of toxic training environments featuring abusive body shaming are needed [34]. The set-up of an interdisciplinary network of trained medical staff including sport and exercise physicians, sports nutritionists and psychologists as well as integrating the family and the coach staff is crucial for the success of therapy from REDs but also for its prevention [4,34]. The more REDs we could prevent, the higher the amount of positive athletic progressions and long-term success we might experience.
Corresponding author
Joëlle Leonie Flueck, Dr. sc. nat.
Swiss Sports Nutrition Society
Fabrikweg 11
8910 Affoltern am Albis
joelle.flueck@ssns.ch

References
- Nattiv A, Loucks AB, Manore MM, Sanborn CF, Sundgot-Borgen J, Warren MP. American College of Sports Medicine position stand. The female athlete triad. Med Sci Sports Exerc. 2007;39(10):1867-82.
- Drinkwater BL, Nilson K, Ott S, Chesnut CH. Bone mineral density after resumption of menses in amenorrheic athletes. JAMA. 1986; 256(3):380-2.
- Mountjoy M, Sundgot-Borgen J, Burke L, Carter S, Constantini N, Lebrun C, et al. The IOC consensus statement: beyond the Female Athlete Triad–Relative Energy Deficiency in Sport (RED-S). Br J Sports Med. 2014;48(7):491-7.
- Mountjoy M, Sundgot-Borgen JK, Burke LM, Ackerman KE, Blauwet C, Constantini N, et al. IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. Br J Sports Med. 2018; 52(11):687-97.
- Wells KR, Jeacocke NA, Appaneal R, Smith HD, Vlahovich N, Burke LM, et al. The Australian Institute of Sport (AIS) and National Eating Disorders Collaboration (NEDC) position statement on disordered eating in high performance sport. Br J Sports Med. 2020;54(21):1247-58.
- Fahrenholtz IL, Melin AK, Wasserfurth P, Stenling A, Logue D, Garthe I, et al. Risk of Low Energy Availability, Disordered Eating, Exercise Addiction, and Food Intolerances in Female Endurance Athletes. Front Sports Act Living. 2022;4:869594.
- Burke LM, Lundy B, Fahrenholtz IL, Melin AK. Pitfalls of Conducting and Interpreting Estimates of Energy Availability in Free-Living Athletes. Int J Sport Nutr Exerc Metab. 2018;28(4):350-63.
- Loucks AB, Kiens B, Wright HH. Energy availability in athletes. J Sports Sci. 2011;29 Suppl 1:S7-15.
- Loucks AB. Energy balance and body composition in sports and exercise. J Sports Sci. 2004;22(1):1-14.
- Heikura IA, Stellingwerff T, Areta JL. Low energy availability in female athletes: From the lab to the field. Eur J Sport Sci. 2022;22(5):709-19.
- Kuikman MA, Mountjoy M, Stellingwerff T, Burr JF. A Review of Nonpharmacological Strategies in the Treatment of Relative Energy Deficiency in Sport. Int J Sport Nutr Exerc Metab. 2021;31(3):268-75.
- Stice E, South K, Shaw H. Future directions in etiologic, prevention, and treatment research for eating disorders. J Clin Child Adolesc Psychol. 2012;41(6):845-55.
- Sundgot-Borgen J, Meyer NL, Lohman TG, Ackland TR, Maughan RJ, Stewart AD, et al. How to minimise the health risks to athletes who compete in weight-sensitive sports review and position statement on behalf of the Ad Hoc Research Working Group on Body Composition, Health and Performance, under the auspices of the IOC Medical Commission. Br J Sports Med. 2013;47(16):1012-22.
- Holtzman B, Ackerman KE. Measurement, Determinants, and Implications of Energy Intake in Athletes. Nutrients. 2019;11(3).
- Melin AK, Areta JL, Heikura IA, Stellingwerff T, Torstveit MK, Hackney AC. Direct and indirect impact of low energy availability on sports performance. Scand J Med Sci Sports. 2023.
- Stenqvist TB, Melin AK, Garthe I, Slater G, Paulsen G, Iraki J, et al. Prevalence of Surrogate Markers of Relative Energy Deficiency in Male Norwegian Olympic-Level Athletes. Int J Sport Nutr Exerc Metab. 2021;31(6):497-506.
- Oxfeldt M, Phillips SM, Andersen OE, Johansen FT, Bangshaab M, Risikesan J, et al. Low energy availability reduces myofibrillar and sarcoplasmic muscle protein synthesis in trained females. J Physiol. 2023.
- Areta JL, Burke LM, Camera DM, West DW, Crawshay S, Moore DR, et al. Reduced resting skeletal muscle protein synthesis is rescued by resistance exercise and protein ingestion following short-term energy deficit. Am J Physiol Endocrinol Metab. 2014;306(8):E989-97.
- Dipla K, Kraemer RR, Constantini NW, Hackney AC. Relative energy deficiency in sports (RED-S): elucidation of endocrine changes affecting the health of males and females. Hormones (Athens). 2021;20(1):35-47.
- Areta JL, Taylor HL, Koehler K. Low energy availability: history, definition and evidence of its endocrine, metabolic and physiological effects in prospective studies in females and males. Eur J Appl Physiol. 2021;121(1):1-21.
- Whitney KE, Holtzman B, Cook D, Bauer S, Maffazioli GDN, Parziale AL, et al. Low energy availability and impact sport participation as risk factors for urinary incontinence in female athletes. J Pediatr Urol. 2021;17(3):290.e1-.e7.
- Melin A, Tornberg Å, Skouby S, Møller SS, Sundgot-Borgen J, Faber J, et al. Energy availability and the female athlete triad in elite endurance athletes. Scand J Med Sci Sports. 2015;25(5):610-22.
- Sim A, Burns SF. Review: questionnaires as measures for low energy availability (LEA) and relative energy deficiency in sport (RED-S) in athletes. J Eat Disord. 2021;9(1):41.
- De Souza MJ, Lee DK, VanHeest JL, Scheid JL, West SL, Williams NI. Severity of energy-related menstrual disturbances increases in proportion to indices of energy conservation in exercising women. Fertil Steril. 2007;88(4):971-5.
- Mallinson RJ, Williams NI, Olmsted MP, Scheid JL, Riddle ES, De Souza MJ. A case report of recovery of menstrual function following a nutritional intervention in two exercising women with amenorrhea of varying duration. J Int Soc Sports Nutr. 2013;10:34.
- Siedler MR, De Souza MJ, Albracht-Schulte K, Sekiguchi Y, Tinsley GM. The Influence of Energy Balance and Availability on Resting Metabolic Rate: Implications for Assessment and Future Research Directions. Sports Med. 2023.
- Arends JC, Cheung MY, Barrack MT, Nattiv A. Restoration of menses with nonpharmacologic therapy in college athletes with menstrual disturbances: a 5-year retrospective study. Int J Sport Nutr Exerc Metab. 2012;22(2):98-108.
- Loucks AB, Verdun M, Heath EM. Low energy availability, not stress of exercise, alters LH pulsatility in exercising women. J Appl Physiol (1985). 1998;84(1):37-46.
- Loucks AB, Thuma JR. Luteinizing hormone pulsatility is disrupted at a threshold of energy availability in regularly menstruating women. J Clin Endocrinol Metab. 2003;88(1):297-311.
- Fahrenholtz IL, Sjödin A, Benardot D, Tornberg Å, Skouby S, Faber J, et al. Within-day energy deficiency and reproductive function in female endurance athletes. Scand J Med Sci Sports. 2018;28(3):1139-46.
- Melin A, Tornberg Å B, Skouby S, Møller SS, Faber J, Sundgot-Borgen J, et al. Low-energy density and high fiber intake are dietary concerns in female endurance athletes. Scand J Med Sci Sports. 2016;26(9):1060-71.
- Sale C, Elliott-Sale KJ. Nutrition and Athlete Bone Health. Sports Med. 2019;49(Suppl 2):139-51.
- Thompson A, Petrie T, Anderson C. Eating disorders and weight control behaviors change over a collegiate sport season. J Sci Med Sport. 2017;20(9):808-13.
- Ackerman KE, Stellingwerff T, Elliott-Sale KJ, Baltzell A, Cain M, Goucher K, et al. #REDS (Relative Energy Deficiency in Sport): time for a revolution in sports culture and systems to improve athlete health and performance. Br J Sports Med. 2020;54(7):369-70.




 nach Ruptur: (K)ein Mysterium mit dem Cross Bracing Protocol® (CBP)")
Comments are closed.